
Thu, Dec 25, 2025

Volume 19, Issue 1 (Jan-Feb 2025)
mljgoums 2025, 19(1): 9-11 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
. S, Jamal I, Choudhary V. Hairy cell leukemia: A case report of unusual presentation without splenomegaly. mljgoums 2025; 19 (1) :9-11
URL: http://mlj.goums.ac.ir/article-1-1619-en.html
URL: http://mlj.goums.ac.ir/article-1-1619-en.html



1- Department Of Pathology (Hematology), Indira Gandhi Institute of Medical Sciences (IGIMS), Patna, India
2- Department Of Pathology (Hematology), Indira Gandhi Institute of Medical Sciences (IGIMS), Patna, India ,iffatjamal111@gmail.com
2- Department Of Pathology (Hematology), Indira Gandhi Institute of Medical Sciences (IGIMS), Patna, India ,
Full-Text [PDF 323 kb]
(1143 Downloads)
| Abstract (HTML) (4636 Views)
Discussion
Splenomegaly is by far the most constant physical finding in HCL, and HCL is typically included in the differential diagnosis of enlarged spleen. Hence, a case of HCL presenting without splenomegaly puts both the clinician and pathologist in a diagnostic dilemma many times, as these cases show only a small percentage of classical abnormal mononuclear cells with circumferential projections in the peripheral blood, as well as in the bone marrow aspirate (3,4).
HCL commonly presents with pancytopenia or variable cytopenia and is associated with splenomegaly and dry tap on bone marrow aspirate resulting from fibrosis (5). HCL must be included in the differential diagnoses of aplastic anemia, hypoplastic myelodysplastic syndrome, atypical chronic lymphocytic leukemia, B-prolymphocytic leukemia, and idiopathic myelofibrosis (6).
HCL presenting without splenomegaly is rare. It puts both the clinician and pathologist in a diagnostic dilemma, as these cases show only a small percentage of abnormal mononuclear cells in the peripheral blood as well as in the bone marrow aspirate, because bone marrow is affected by bone marrow fibrosis (5). Hence, bone marrow biopsy is the only morphologic tool available for diagnosis of HCL, highlighting the high index of suspicion that a morphologist should have in such cases, as HCL cases without splenomegaly most often have a hypocellular bone marrow, and these cases may be erroneously diagnosed as aplastic anemia. The incidence of HCL without splenomegaly in various series ranged from 0 to 30% (6-12) (Table 1).
Conclusion
This case report highlights the uncommon clinical presentation of HCL without splenomegaly, creating a diagnostic challenge. A careful attention to morphological details in bone marrow biopsy is a prerequisite for its correct and early diagnosis, thereby providing maximum benefit to patients.
Acknowledgement
We are grateful to the patient for providing informed consent and allowing us to share this case.
Funding sources
None.
Ethical statement
This case report was approved by the institution's ethics committee, and all patient information has been anonymized to protect confidentiality.
Conflicts of interest
None declared.
Author contributions
All authors contributed to the conception and design of the case report.
Data availability statement
The data is derived from public domain resources and can be accessed.
Full-Text: (819 Views)
Introduction
Hairy cell leukemia (HCL) is a rare B-cell neoplasm of middle age, presenting with pancytopenia, splenomegaly, and hairy cells in the bone marrow. Splenomegaly accounts for 80-90% of associated features in HCL (1). A careful study of morphological findings on bone marrow aspirate and biopsy, followed by appropriate ancillary tests, aids in correct diagnosis. A high index of suspicion is essential for diagnosing and appropriately managing such cases. A strong suspicion of morphology in such cases is a prerequisite for reaching a correct diagnosis, even without the usual clinical presentation (2). Splenomegaly is by far the most constant physical finding in HCL, and HCL is typically included in the differential diagnosis of splenic enlargement. Hence, a case of HCL presenting without splenomegaly puts both the clinician and pathologist in diagnostic dilemma many times. These cases show only a small percentage of abnormal mononuclear cells in the peripheral blood as well as in the bone marrow aspirate, because bone marrow is usually fibrosed in these cases (3). Hence, bone marrow biopsy is the only morphologic tool available for the diagnosis of HCL, highlighting the high index of suspicion that a morphologist should maintain in such cases. HCL cases without splenomegaly most often have hypocellular bone marrow, and these cases may be erroneously diagnosed as aplastic anemia (4). The incidence of HCL without splenomegaly in various series ranged from 0 to 30% in a few of the case reports described earlier-some series report bone marrow hypocellularity to the tune of 18% (5). Here, we represent an atypical case of HCL with weakness only, but no splenomegaly. This report of an unusual presentation of such a rare disease may lead to an earlier diagnosis of HCL, even in the absence of a typical clinical presentation.
Case presentation
A 48-year-old male presented with a three-month history of weakness and fatigue. On examination, he had pallor; however, he had no organomegaly or lymphadenopathy. He had a history of on and off blood transfusion in the past. Hemogram revealed pancytopenia with hemoglobin - 9.0 gm/dl, total leucocyte count - 3200/cumm, with a differential count revealing 68% hairy cells, which are of intermediate size and have abundant blue cytoplasm, some with circumferential projections; Neutrophils - 12%, Lymphocytes - 18%, Eosinophils - 2%, and platelets - 90000/cumm (Figure 1a). Bone marrow aspiration was carried out for evaluation of pancytopenia. Bone marrow aspiration smears were hypercellular for age and showed infiltration by hairy cells. Other cell lineages were markedly suppressed (Figure 1b and c). Immunophenotyping by flow cytometry revealed a monoclonal small B-cell population with an expression of CD19 (Bright), CD20 (Bright), CD79b (Bright), CD25 (Moderate), CD103 (Moderate to Bright), CD200 (Dim), FMC-7 (Dim), CD11c (Bright), and surface kappa restricted (Moderate) (Figure 1d and e). Subsequently, the patient received standard-dose chemotherapy with cladribine and achieved hematological remission. Due ethical clearance was taken from the institutional ethical committee with reference no. IEC/IGIMS/2345. Written informed consent was taken from the patient.
Hairy cell leukemia (HCL) is a rare B-cell neoplasm of middle age, presenting with pancytopenia, splenomegaly, and hairy cells in the bone marrow. Splenomegaly accounts for 80-90% of associated features in HCL (1). A careful study of morphological findings on bone marrow aspirate and biopsy, followed by appropriate ancillary tests, aids in correct diagnosis. A high index of suspicion is essential for diagnosing and appropriately managing such cases. A strong suspicion of morphology in such cases is a prerequisite for reaching a correct diagnosis, even without the usual clinical presentation (2). Splenomegaly is by far the most constant physical finding in HCL, and HCL is typically included in the differential diagnosis of splenic enlargement. Hence, a case of HCL presenting without splenomegaly puts both the clinician and pathologist in diagnostic dilemma many times. These cases show only a small percentage of abnormal mononuclear cells in the peripheral blood as well as in the bone marrow aspirate, because bone marrow is usually fibrosed in these cases (3). Hence, bone marrow biopsy is the only morphologic tool available for the diagnosis of HCL, highlighting the high index of suspicion that a morphologist should maintain in such cases. HCL cases without splenomegaly most often have hypocellular bone marrow, and these cases may be erroneously diagnosed as aplastic anemia (4). The incidence of HCL without splenomegaly in various series ranged from 0 to 30% in a few of the case reports described earlier-some series report bone marrow hypocellularity to the tune of 18% (5). Here, we represent an atypical case of HCL with weakness only, but no splenomegaly. This report of an unusual presentation of such a rare disease may lead to an earlier diagnosis of HCL, even in the absence of a typical clinical presentation.
Case presentation
A 48-year-old male presented with a three-month history of weakness and fatigue. On examination, he had pallor; however, he had no organomegaly or lymphadenopathy. He had a history of on and off blood transfusion in the past. Hemogram revealed pancytopenia with hemoglobin - 9.0 gm/dl, total leucocyte count - 3200/cumm, with a differential count revealing 68% hairy cells, which are of intermediate size and have abundant blue cytoplasm, some with circumferential projections; Neutrophils - 12%, Lymphocytes - 18%, Eosinophils - 2%, and platelets - 90000/cumm (Figure 1a). Bone marrow aspiration was carried out for evaluation of pancytopenia. Bone marrow aspiration smears were hypercellular for age and showed infiltration by hairy cells. Other cell lineages were markedly suppressed (Figure 1b and c). Immunophenotyping by flow cytometry revealed a monoclonal small B-cell population with an expression of CD19 (Bright), CD20 (Bright), CD79b (Bright), CD25 (Moderate), CD103 (Moderate to Bright), CD200 (Dim), FMC-7 (Dim), CD11c (Bright), and surface kappa restricted (Moderate) (Figure 1d and e). Subsequently, the patient received standard-dose chemotherapy with cladribine and achieved hematological remission. Due ethical clearance was taken from the institutional ethical committee with reference no. IEC/IGIMS/2345. Written informed consent was taken from the patient.
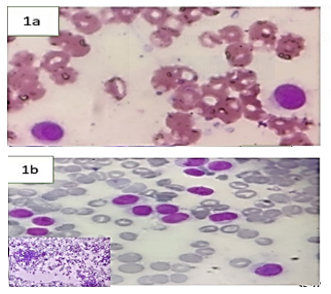 |
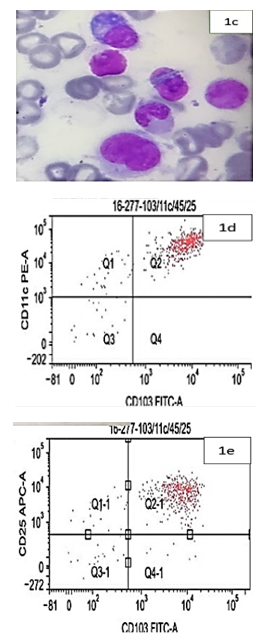 Figure 1. a: Peripheral blood smear showing atypical lymphoid cells with circumferential projections (x100X). b: Bone marrow aspirate showing infiltration by atypical lymphoid cells (x40X). Inset shows hypercellular marrow (x10X). c: Bone marrow aspirate showing lymphoid cells with cytoplasmic projections (x100X). d and e: Flow cytometry revealing bright expression of CD11c and moderate expression of CD103 and CD25. |
Discussion
Splenomegaly is by far the most constant physical finding in HCL, and HCL is typically included in the differential diagnosis of enlarged spleen. Hence, a case of HCL presenting without splenomegaly puts both the clinician and pathologist in a diagnostic dilemma many times, as these cases show only a small percentage of classical abnormal mononuclear cells with circumferential projections in the peripheral blood, as well as in the bone marrow aspirate (3,4).
HCL commonly presents with pancytopenia or variable cytopenia and is associated with splenomegaly and dry tap on bone marrow aspirate resulting from fibrosis (5). HCL must be included in the differential diagnoses of aplastic anemia, hypoplastic myelodysplastic syndrome, atypical chronic lymphocytic leukemia, B-prolymphocytic leukemia, and idiopathic myelofibrosis (6).
HCL presenting without splenomegaly is rare. It puts both the clinician and pathologist in a diagnostic dilemma, as these cases show only a small percentage of abnormal mononuclear cells in the peripheral blood as well as in the bone marrow aspirate, because bone marrow is affected by bone marrow fibrosis (5). Hence, bone marrow biopsy is the only morphologic tool available for diagnosis of HCL, highlighting the high index of suspicion that a morphologist should have in such cases, as HCL cases without splenomegaly most often have a hypocellular bone marrow, and these cases may be erroneously diagnosed as aplastic anemia. The incidence of HCL without splenomegaly in various series ranged from 0 to 30% (6-12) (Table 1).
Conclusion
This case report highlights the uncommon clinical presentation of HCL without splenomegaly, creating a diagnostic challenge. A careful attention to morphological details in bone marrow biopsy is a prerequisite for its correct and early diagnosis, thereby providing maximum benefit to patients.
Acknowledgement
We are grateful to the patient for providing informed consent and allowing us to share this case.
Funding sources
None.
Ethical statement
This case report was approved by the institution's ethics committee, and all patient information has been anonymized to protect confidentiality.
Conflicts of interest
None declared.
Author contributions
All authors contributed to the conception and design of the case report.
Data availability statement
The data is derived from public domain resources and can be accessed.
Research Article: Case Report |
Subject:
Laboratory Sciences
Received: 2023/02/2 | Accepted: 2023/05/22 | Published: 2025/01/27 | ePublished: 2025/01/27
Received: 2023/02/2 | Accepted: 2023/05/22 | Published: 2025/01/27 | ePublished: 2025/01/27
References
1. Zoldan MC, Ponzoni M, Ricci D, Camba L, Faravelli A. Hairy cell leukemia without splenomegaly nor myelofibrosis in a patient with gastric adenocarcinoma: early phase of the disease or a variant? Pathologica. 1995; 87(1): 97-9. [View at Publisher] [PMID] [Google Scholar]
2. Muta T, Okamura T, Oshima K, Kikuchi M, Niho Y. European-American-type hairy cell leukemia without splenomegaly, treated successfully with deoxycoformycin. Rinsho. 2001; 42(5): 426-31. [View at Publisher] [PMID] [Google Scholar]
3. Spedini P, Tajana M, Bergonzi C. Unusual presentation of hairy cell leukemia. Haematologica. 2000; 85(5): 548. [View at Publisher] [PMID] [Google Scholar]
4. Westbrook CA, Golde DW. Clinical problems in hairy cell leukemia: diagnosis and management. Semin Oncol. 1984; 11(4 Suppl 2): 514-22. [View at Publisher] [PMID] [Google Scholar]
5. Karmali R, Farhat M, Leslie W, McIntire MG, Gregory S. Localized bone disease as a presentation of hairy cell leukemia. Clin Adv Hematol Oncol. 2008; 6(4): 290–294. [View at Publisher] [PMID] [Google Scholar]
6. Burke JS,Byrne G, Appaport H. Hairy cell leukemia(leukemic reticuloendotheliosis). A clinical pathologic study of 21 patients. Cancer. 1974; 33: 1394-1410. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Bouroncle BA. Leukemic reticuloendotheliosis (hairy cell leukemia). Blood. 1979; 53(3): 412-36. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Chatterjee T, Panigrahi I, Mahapatra M, Pati HP, Kumar R, Naithani R, et al. Hairy cell leukemia: clinical, pathological and ultrastructural findings in Asian-Indians. Indian J Cancer. 2008; 45(2): 41-4. [View at Publisher] [DOI] [PMID] [Google Scholar]
9. Bhargava R, Kar R, Mahapatra M, Saxena R. The clinico-hematological profile of hairy cell leukaemia: a single centre experience. Hematology. 2010; 15(3): 162-4. [View at Publisher] [DOI] [PMID] [Google Scholar]
10. Galani KS, Subramanian PG, Gadage VS, Rahman K, Ashok Kumar MS, Shinde S, et al. Clinico-pathological profile of Hairy cell leukemia: critical insights gained at a tertiary care cancer hospital. Indian J Pathol Microbiol. 2012; 55: 61-65. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Găman AM. Hairy cell leukemia--a rare type of leukemia. A retrospective study on 39 patients. Rom J Morphol Embryol. 2013; 54(3): 575-9. [View at Publisher] [PMID] [Google Scholar]
12. Venkatesan S, Purohit A, Aggarwal M, Manivannan P, Tyagi S, Mahapatra M, et al. Unusual presentation of hairy cell leukemia: a case series of four clinically unsuspected cases. Indian J Hematol Blood Transfus. 2014; 30(Suppl 1): 413-7. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.

Contact us
Tel & Fax: (+98) 17-32450093
E-mail:
 goums.ac.ir
goums.ac.ir yahoo.com
yahoo.com